
As conversational AI systems become more integrated into everyday life, an important question remains: how do people actually experience these systems in real-world, culturally diverse contexts?
At YUX, we’ve been exploring this question through an ongoing research initiative, in collaboration with the Gates Foundation, focused on evaluating multilingual Voice-to-Voice (V2V) AI systems for health-related self-care in Senegal and Rwanda. The project explores whether AI voice systems are actually useful and viable for healthcare support in low-resource and multilingual contexts, while also examining how trust, language, culture, and lived experience shape people’s interactions with these systems.
Unlike traditional text-based chatbots, V2V systems process speech directly to speech, preserving conversational elements such as tone, pacing, emotion, and turn-taking. These qualities are especially important in health and caregiving contexts, where reassurance, empathy, and trust influence how people interpret and act on information. Voice interaction may also help reduce barriers for lower-literacy populations, allowing participants to speak naturally in the languages they are most comfortable with.
However, while these systems seem promising, several important questions remain:
- Can these systems actually be trusted in health-related situations?
- Is the advice contextually relevant to people’s lived realities?
- Can the systems accurately understand local languages and code-switching?
- How do people perceive the tone, clarity, and usefulness of AI-generated voice responses?
These questions are especially important because much of today’s AI evaluation still focuses mainly on benchmark performance, technical accuracy, and safety metrics. While these are important, they often fail to capture how people actually interpret, negotiate, trust, and evaluate AI systems within real social and cultural environments. This challenge is particularly relevant in African contexts characterized by multilingual interaction, varying levels of digital familiarity, and complex healthcare realities.
The project currently focuses on three health-related self-care areas:
- Maternal, Child, and Reproductive Health (MCRH)
- Symptom Triaging
- Chronic Care Support (including TB and HIV)
Our research is guided by the following questions:
- What are the practical abilities and limitations of current V2V AI systems in health-related self-care interactions?
- In which self-care use cases does V2V AI demonstrate the strongest real-world usefulness and viability?
- How do user characteristics such as digital access, language, and health-seeking behaviors influence interactions with these systems?
- Which user-centered metrics best capture the perceived usefulness and real-world value of V2V AI systems?
- How does V2V AI performance vary across languages and code-switching contexts?
To explore these questions, the study combines multiple participatory and human-centered evaluation methods designed to move beyond conventional AI benchmarking approaches.
Step 1: Expert Consultations:

The project began with expert consultation sessions involving healthcare professionals including doctors, nurses, pharmacists, community health workers, and public health specialists. These sessions helped identify key themes across the different use cases, map common health-seeking pathways, and define evaluation criteria for assessing V2V AI responses within local healthcare contexts.
The expert consultations also played an important role in refining the evaluation metrics and identifying potential safety concerns, cultural considerations, and realistic healthcare constraints relevant to both Senegal and Rwanda.
Step 2: Cultural Teaming:

One of the central methods used in the study is Cultural Teaming, adapted from participatory red-teaming methodologies and inspired by the work of Chiu et al. (2024).
These workshops are designed to evaluate AI-generated health advice within realistic, everyday contexts. Participants work in pairs and engage directly with the V2V AI systems through open-ended conversations related to themes identified during the expert consultation phase. Participants are also guided using adversarial nudges designed to surface more complex, culturally situated, or emotionally sensitive situations.
Following each interaction, participants evaluate the responses based on factors such as trust, clarity, tone, usefulness, and contextual appropriateness. The sessions also include group reflections and discussions around what worked well, where the systems struggled, and how the interactions could be improved.
Step 3: Diary Studies:
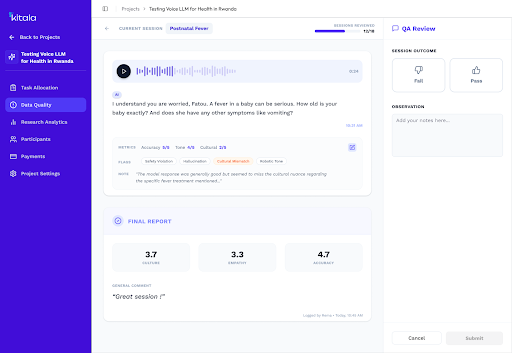
To complement the in-depth qualitative and adversarial insights from the Cultural Teaming sessions, the project also includes diary studies conducted through Kitala, YUX’s in-house AI evaluation platform.
Participants interact with the V2V systems over multiple days using their personal smartphones and provide evaluations after each interaction. The goal is to better understand how people engage with AI systems over time within more naturalistic settings outside of facilitated workshops, but in a controlled / safe environment.
Step 4: Health Expert Review:
As part of the methodology, a subset of participant audio interactions from the Cultural Teaming and diary study phases are also reviewed by healthcare professionals through a blind expert review process.
These experts assess the conversations from a clinical and contextual perspective, helping the team compare participant perceptions with clinical interpretations around issues such as safety, usefulness, clarity, and contextual realism. This allows the research to examine where lived experience and clinical evaluation align and where they may differ.
Methodological learnings so far:
The pilot phase of the study has already generated important methodological learnings around how to evaluate AI systems in real-world, multilingual, and low-resource contexts.
- Participants don't think like researchers: One of the strongest findings from the pilot was that participants, particularly those with lower literacy or limited familiarity with AI, struggled to consistently interpret researcher-defined evaluation metrics such as Likert scales and abstract quality dimensions. This suggests that future evaluations should rely on simpler, more intuitive feedback mechanisms that reduce participant burden while preserving both qualitative and quantitative insights.
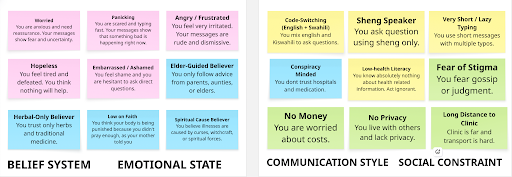
- Precise participant segmentation strengthens AI evaluation but increases operational complexity: Digital Personas and the pathways segmentation provided meaningful structure for understanding differences in technology use, health-seeking behaviors, and evaluation experiences across participant groups. At the same time, the pilot highlighted the practical challenges of recruiting underrepresented groups, particularly lower-connectivity populations, emphasizing the need for broader recruitment strategies and approaches in future studies.
- Facilitated evaluation remains important in low-resource settings: Although voice interaction reduced some literacy barriers, participants still required substantial onboarding and support to confidently engage with V2V systems. Facilitator-supported Cultural Teaming sessions proved essential for enabling meaningful participation, suggesting that independent evaluation may not yet be appropriate across all user groups and contexts.
- Multi-turn conversations require lightweight evaluation approaches: Repeated evaluation after every conversational turn interrupted the natural flow of interactions and increased participant fatigue. The pilot suggests that longer conversational evaluations should prioritize lightweight interaction markers and post-conversation reflection rather than repeated detailed ratings throughout the interaction.
- Quality assurance should prioritize analysis over exclusion: A significant portion of the collected sessions were excluded through the initial QA process because they did not fully meet predefined evaluation criteria. While ensuring data quality remains important, the pilot highlighted that many rejected conversations still contained valuable information about model failures, participant behavior, and interaction patterns. Future work will complement traditional QA with analytical frameworks that distinguish between successful interactions, recoverable failures, and unsafe conversations rather than treating them simply as valid or invalid.
- Behavioral outcomes may be more meaningful than satisfaction ratings: The pilot highlighted an important distinction between participants enjoying an interaction and being willing to act upon the advice received. Future evaluations will move beyond satisfaction-focused measures toward behavioral outcomes, such as intended next actions, confidence in decision-making, and the role of trust in shaping health-seeking behaviors.
- Conversational qualities deserve dedicated evaluation: Beyond factual correctness, participants consistently reflected on tone, empathy, authority, and conversational flow when describing their experiences with the system. Future evaluation frameworks will explicitly examine how conversational qualities shape trust, perceived credibility, and willingness to engage with V2V systems over time.
